Mon, Jul 6, 2026
Volume 11 - Continuous Publishing
Iran J Neurosurg 2025, 11 - Continuous Publishing: 0-0 |
Back to browse issues page
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Modaenama M, alijani B, Reihanian Z, Jafari S. Prognostic value of NLR in adult patients with hydrocephalus treated with an external ventricular drain: a retrospective study. Iran J Neurosurg 2025; 11 : 14
URL: http://irjns.org/article-1-487-en.html
URL: http://irjns.org/article-1-487-en.html



1- Neuroscience Research Center, Trauma Institute, Guilan University of Medical Sciences, Rasht, Iran
2- Guilan Road Trauma Research Center, Trauma Institute, Guilan University of Medical Sciences, Rasht, Iran. & Department of Neurosurgery, School of Medicine, Poursina Hospital, Guilan University of Medical Sciences, Rasht, Iran
3- Department of Neurosurgery, School of Medicine, Poursina Hospital, Guilan University of Medical Sciences, Rasht, Iran.
2- Guilan Road Trauma Research Center, Trauma Institute, Guilan University of Medical Sciences, Rasht, Iran. & Department of Neurosurgery, School of Medicine, Poursina Hospital, Guilan University of Medical Sciences, Rasht, Iran
3- Department of Neurosurgery, School of Medicine, Poursina Hospital, Guilan University of Medical Sciences, Rasht, Iran.
Full Text [PDF 2096 kb]
(231 Downloads)
| Abstract (HTML) (958 Views)
Full Text: (156 Views)
1. Introduction
Hydrocephalus is the leading cause of neurosurgical conditions globally, which involves the expansion of the brain ventricles filled with cerebrospinal fluid (CSF) as a result of impaired CSF homeostasis, culminating in progressive dilation of the brain ventricular system [1]. Regardless of the cause, hydrocephalus is frequently defined by elevated intracranial pressure, enlarged ventricular chambers from CSF accumulation, and brain structural damage, which can lead to neurological deterioration, coma, and death if not treated [2]. When hydrocephalus is diagnosed, CSF diversion is required to keep normal cerebral pressure. The insertion of an external ventricular drain (EVD) is the initial therapy for acute hydrocephalus, allowing for the diversion and control of excess CSF, dependent on the total drainage status, to mitigate the related rise in intracranial pressure, which, if left untreated, may contribute to lower brain circulation and later neurological impairment [3].
Several studies have found brain and CSF inflammation after EVD treatment in both posthemorrhagic and postinfectious hydrocephalus [4]. Although the restoration of inflammatory responses is critical for the removal of invading pathogens, damaged cells, and irritating substances, it can also develop or promote the disease if it is incorrectly induced or prolonged. The presence of multiple inflammatory agents in the circulatory system or CSF has been linked to an increased risk for post-hemorrhagic or post-infectious hydrocephalus, as well as a greater degree of symptoms [5]. There is accumulating evidence that an immune-related inflammation in the central nervous system (CNS) is a major cause of initial posttraumatic cerebral damage and related clinical outcomes [6]. According to experimental and clinical research, EVD activates and proliferates several leukocyte subtypes (e.g. neutrophils, lymphocytes) in mouse models and humans with hydrocephalus [7, 8]. High neutrophil counts stimulate the neuro-inflammation pathway, exacerbating edema and hematoma formation, increasing mass impact and intracranial pressure, and resulting in nervous system impairment [9]. Lymphocytes, as an adaptive immune response, are necessary for bodily defense, and low lymphocyte counts imply a worse prognosis in hydrocephalus patients with an increased incidence of infections [10].
The neutrophil-to-lymphocyte ratio (NLR) has been suggested as a valid compound indicator and dynamic scale of the inflammatory process by calculating total neutrophil and lymphocyte numbers [11]. The NLR represents the immune response and integrates data from both the innate and adaptive. In addition, since counts of neutrophils and lymphocytes are frequently evaluated during laboratory tests, the NLR is useful in clinical settings. NLR has been widely studied and found to be linked with consequences, with high NLR having prognostic value for numerous disorders, such as cardiovascular disease [12], ischemic stroke [13], cerebral hemorrhage [14], and infectious diseases [15]. Furthermore, greater NLR is linked to a worse prognosis in cancer patients [16]. These negative connections could be related to the roles of excessive inflammation and impaired immunological activity in the course of these disorders. As a result, NLR is a helpful indicator of vulnerability to subsequent brain injury and post-stroke problems caused by increased neutrophils and decreased lymphocytes [17]. There is evidence that patients with higher neutrophil levels and lower lymphocyte levels had less favorable outcomes in ischemic and hemorrhagic strokes [18]. These results suggest that assessing the NLR in the CSF of patients with hydrocephalus may be especially important because inflammatory responses emerge to have a substantial impact on prognosis following EVD treatment. NLR may thus be predictive of death in hydrocephalus patients, as well as the general influence of inflammation and the immune system on health. A better understanding of the relationship between NLR and critical clinical factors on mortality rate would assist in elucidating the function of inflammation and immune response in the progression and consequences of many diseases. While several studies have examined the predictive usefulness of NLR in terms of mortality rates because of cancer, cardiac disease, or stroke, no research has examined such relationships in the context of hydrocephalus. The present study examines the connections of the NLR combined with significant clinical parameters with overall mortality and prognosis in the CSF of patients with hydrocephalus after EVD to provide more support information for hydrocephalus management.
2. Methods and Materials/Patients
Study design
We conducted a cross-sectional study on 40 consecutive hydrocephalus patients who underwent EVD insertions in the Neurosurgery Ward of Poursina Hospital in Rasht City, Iran, January 2020 and December 2022. The Ethics Committee of the hospital approved the study design. All patients or their families provided informed consent. In addition, a convenient means of sampling was selected in this research.
Patient selection
The inclusion criteria were as follows: 1) all patients with hydrocephalus on admission computed tomography (CT) who had EVD insertion and a CSF sample taken from the surgical site; 2) patient age ≥18 years; 3) the duration of intensive care unit (ICU) and hospitalization, as well as short-term mortality (death occurred before hospital discharge) were recorded; 4) first CSF specimen for laboratory tests 24 h after admission; 5) white blood cell count greater than 5 in CSF sample and cell index greater than 1 in case of intraventricular hemorrhage(IVH).
In addition, the exclusion crieteria included the following items: 1) the lack of laboratory results for testing 24 h after admission; 2) <4 days survival from the onset of symptoms; 3) individuals who had surgery before the 24-h CT; 4) past cerebral abnormalities such as ischemia or hemorrhagic stroke; 5) immunodeficiency or autoimmune disorders; 6) hematologic diseases and tumors; 7) a history of systemic problems, such as uremia, liver cirrhosis, chronic heart or lung disease; 8) patients who met the inclusion criteria but had insufficient data on their charts. Medical records were used to obtain clinical data and imaging scans for each patient, and an online pathology registry was used to collect microbiology and biochemistry reports. The data from the patients were then retrospectively analyzed, and a variety of parameters (detailed in the following sections) were evaluated.
EVD indications
The EVD was inserted on the clinically preferred side. The clinical indication determined the EVD height, which was opened to drainage when the intracranial pressure exceeded a threshold of 20 mmHg. Clinical manifestations (such as mental status changes, lethargy, somnolence, or pupillary alterations) and radiographic data indicating acute hydrocephalus (such as ventriculomegaly, increase in temporal horn size, cisternal effacement, or sulcal effacement) were both considered when deciding whether or not to insert an EVD at the time of admission. Lumbar drains were not employed to divert CSF.
Parameters in clinical and laboratory settings
Patients were divided into two groups: Subjects who were alive (n=20) and subjects who were dead (n=20). We analyzed demographic data (age, gender), clinical status (level of consciousness, underlying disease, type of primary disease, and history of COVID-19 and organ failure), and laboratory data (neutrophil, lymphocyte, and NLR) collected from CSF 24 h after admission. An autoanalyzer was used to measure the number of white blood cells, neutrophils, and lymphocytes. Our hospital laboratory equipment was used to conduct an absolute neutrophil count (ANC) and absolute lymphocyte count (ALC). NLR was then determined using the ANC/ALC methodology.
Statistical analysis
The demographic data is demonstrated in a table format, with numerical parameters using the Mean±SD and categorical factors using numbers and percentages. The Fisher exact test for proportions, the Student t-test for continuous normally distributed data, and the Mann-Whitney test for non-normally distributed continuous data were used for comparing baseline features in those who had or did not have an event of death before discharge. To generate the clinical significance of an odds ratio (OR) with 95% confidence intervals (CI), outcome factors were examined using adjusted and unadjusted data in simple and multiple logistic regression models. Multiple logistic regression models were employed to examine the relationship between mortality and clinically significant prognostic markers, such as age, underlying disease, level of consciousness, and NLR. To demonstrate the predictive properties of various laboratory measurements related to mortality, receiver operating characteristic (ROC) curves were designed. The Binomial exact method was used to investigate the risk of mortality related to critical parameters and calculate the CI for the area under the curve (AUC). Furthermore, the DeLong et al. test was employed to determine the statistically significant variations between curves. Meanwhile, P<0.05 were used to determine statistical significance. All statistical analyses were carried out using IBM SPSS software, version 21.0, MedCalc software, version 20.026, and GraphPad Prism software, version 9.0.0.
3. Results
We examined patient database entries from 2020 to 2022. A total of 40 patients with hydrocephalus who were treated surgically with EVD insertion for CSF diversion on admission and met the inclusion criteria were found, for whom follow-up data were available. The baseline demographic and clinical characteristics of patients diagnosed with acute symptomatic hydrocephalus are summarized in Table 1. As previously stated, the patients were separated into two groups: Dead (n=20) and alive (n=20). All patients were adults, with mean ages ranging from 22 to 78 years (51.68±16.34; P=0.038), and there were more males in the population (60%). Median glasgow coma score (GCS) on admission ranged from 3 to 13, with a Mean±SD of 7.10±2.39, and 24 patients (60%) presented with a GCS<8. The median presentation GCS in alive patients was 8.85 (6-13) in comparison to 5.35 (3-8) in dead patients (P≤0.001). The median duration of ICU admission was 6.5 days, and that of overall hospital stay was 14 days; days with an EVD were not different between groups. Overall, mortality was 20 from 40 cases (50%). More than half of the patients had an intracranial hemorrhage (55%), whereas about a fifth had no history of COVID-19 or organ failure and underlying disease (82.5% and 80%, respectively). The mean NLR in our entire study was 6.77±5.55. Patients who died showed greater NLRs than those who were alive, with median NLRs of 8.49 vs 5.05, respectively (P=0.027).
.PNG)
.PNG)
ROC curve
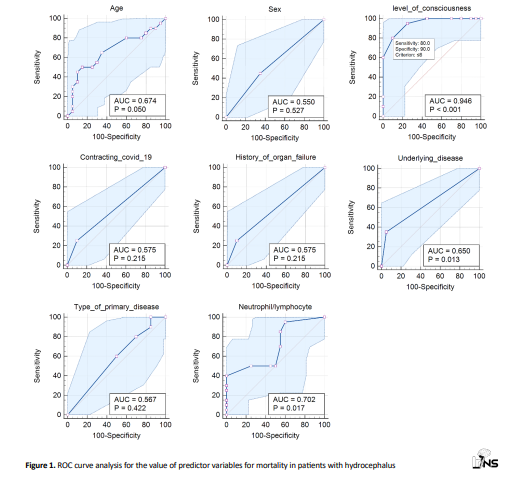
To assess the predictive potential of the selected indicators, ROC curves were provided. Actual NLR results on the value of markers on admission for hydrocephalus indicated an appropriate AUC (AUC=0.702, 95% CI, 0.537 %, 0.836%; P=0.0171; Figure 1). The optimal NLR threshold value for predicting mortality rate was 8.88 with a sensitivity and specificity of 40% and 100%, respectively. In addition, the actual values of underlying disease (AUC=0.650; 95% CI, 0.483%, 0.794%; P=0.0126), consciousness level (AUC=0.946; 95% CI, 0.825%, 0.993%; P<0001), and age (AUC=0.674; 95% CI, 0.507%, 0.813%; P=0.0496) potentially predict mortality, while classified values of other clinical factors appear to be poor predictors (Figure 1). Table 2 analyzes the relationship between NLR and important factors in both patient groups who died and those who did not survive. The correlation of NLR with the level of consciousness was statistically significant (CI, 0.0761%, 0.411%; P=0.0044). In contrast, there was no significant difference in patients with NLR related to age and underlying disease.
.PNG)
NLR correlation with factors predicting mortality and clinical prognosis
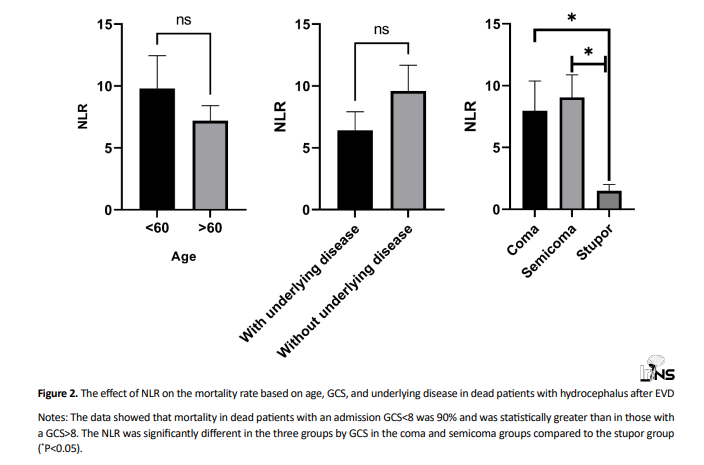
To further analyze the effect of NLR on mortality, the dead group was divided based on age, GCS, and underlying disease. As shown in Figure 2, mortality in patients with an admission GCS<8 was 90% (18/20) and was statistically greater than in those with a GCS>8. The level of consciousness varied from coma (n=4), semicoma (n=14), and stupor (n=2). The GCS scores of coma, semicoma, and stupor were 3.5±0.28, 5.66±0.21, and 8.5±0.5, respectively (Figure 2). The GCS scores did not differ significantly between coma and semicoma levels. GCS scores also increased as the consciousness level increased. NLR was significantly different in the three groups by GCS in coma and semicoma groups compared to the stupor group (P<0.05). Univariate analysis revealed that NLR in age and underlying disease was not significantly correlated with mortality.
Logistic regression
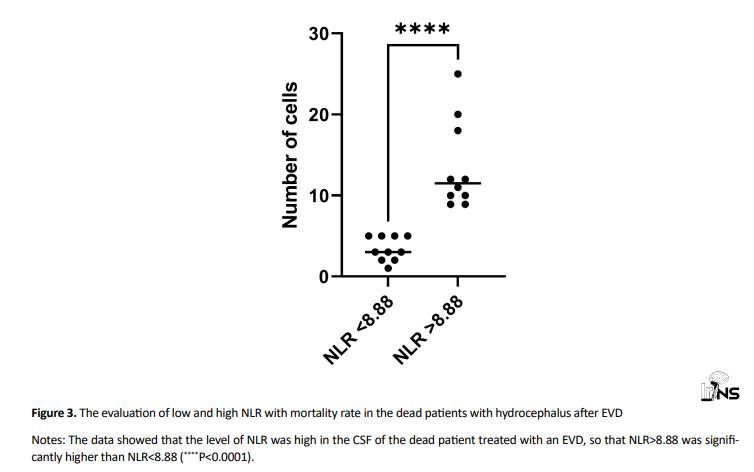
Logistic regression analysis was used to predict unfavorable results using significant univariate characteristics (Table 3). The level of consciousness on admission was associated with mortality (OR=0.23; 95% CI, 0.08 %, 0.65%; P=0.005). According to these regression analyses, there were no significant indicators for sex, age, or overall NLR. We then characterized dead patients based on the rate of NLR (>8.88 vs <8.88) in the CSF. A total of 10 (50%) patients had an NLR<8.88, and 50(50%) >8.88 (P<0.0001; Figure 3). The median GCS in individuals with NLR<8.88 was 5.88, compared to 4.58 in those with NLR>8.88. In addition, the number of patients with GCS<8 was higher than the GCS<8 group. The NLR>8.88 group had a greater mortality rate in terms of coma (30%) and semicoma (70%) (P<0.0001; Table 4).
.PNG)
4. Discussion
To the best of the authors’ knowledge, this is the first study to investigate the connections between high NLR and GSC scores in the CSF of hydrocephalus patients following EVD. In this study, we discovered that a higher NLR combined with GSC score was substantially linked with death, implying that neutrophils and lymphocytes may play a role in the poor prognosis. In the first step, we identified many risk variables for acute symptomatic hydrocephalus after EVD. According to our univariate analysis, the affected patients had a mean age of 51.6 years, with 60% being men. The average age and gender of patients can be important determinants of mortality. According to the findings, comparing the average ages of patients with mortality and surviving patients revealed a significant difference (P=0.038), and the average age of patients with mortality was higher. At older ages, the increase in the probability of mortality in men appears to be inversely proportional to the increase in the probability of discharge, implying that men die more frequently in hospitals [19]. We examined several of these cases, which included primary disease, a history of COVID-19 infection, and organ failure. The findings revealed that more than 80% of the patients did not report a history of organ failure or even the COVID-19 virus. To some extent, these circumstances can mitigate the disturbing effect of organ failure on patient mortality. Furthermore, there was no significant difference in gender between those who died and those who were alive. A similar study found that the general connection between age and premature death is similar in men and women. James et al. examined the relationship between the age and gender of people with cerebral hemorrhage and concluded that as men and women age, the rate of in-hospital death increases slightly more in men than in women [20].
We also discovered that the average level of consciousness in patients who died was lower than in those who were alive (P<0.001). The GCS was the initial objective scoring index used to evaluate patients’ levels of consciousness. According to Teasdale et al. there was a link between GCS score measurement and clinical outcomes, demonstrating a link between a drop in GCS score and an increase in mortality [21]. A low GCS score is an independent predictor of poor prognosis in hemodialysis patients with subarachnoid hemorrhage and traumatic intracranial hemorrhage [22-24]. The GCS score can independently predict hospital mortality; nonetheless, GCS has limitations as a subjective rating tool. For instance, measuring the GCS score in individuals who are sedated, on a ventilator, have jaw and face trauma, or are under the influence of illegal substances or alcohol is problematic [25].
NLR is a biomarker that indicates the equilibrium of the two components of the immune system. It is determined as a simple ratio of the count of neutrophils to lymphocytes in the circulatory system. This ratio is also computed in the CSF. NLR may be a predictor of overall population mortality, as well as the impact of inflammation and immunology on health [26]. Our findings revealed that the average NLR in patients who died was considerably higher than in survivors (P=0.027). The first indication of cerebral hemorrhage is blood flow stagnation, which can be detected both within and surrounding the hematoma. Following that, the blood-brain barrier is disrupted. Endothelial cells, as well as dying neurons and glial cells, release a large number of inflammatory molecules [27, 28]. The first inflammatory cells to enter the site are neutrophils, followed by the activation of lymphocytes as adaptive immune system cells [29]. Therefore, a deeper knowledge of the association between NLR or other clinical indicators and overall mortality in the CSF provides insight into the function of inflammation and immunity in disease development and prognosis. NLR could be used to track patients who have undergone EVD and predict their prognosis and mortality [30]. As a result, we investigated the likelihood of using the biomarkers independent of the thresholds reported in the study. For this purpose, regression analysis as well as ROC curves were used. The ROC curve contrasts the ability of a true-positive rate (sensitivity) and a false-positive rate (specificity) to predict a dichotomous result over a range of values. In our findings, the levels of age, NLR, underlying disease, and level of consciousness were associated with the mortality rate and, as continuous factors, indicated a better AUC. Several studies have been conducted to evaluate the NLR function as a predicted inflammatory biomarker in the mortality rate after EVD [30-32]. Our study was the first to investigate the major characteristics linked with NLR for death rate in patients with hydrocephalus. The present findings revealed that the connection between NLR and the level of consciousness (coma vs stupor group) was much higher in the dead group. A retrospective cohort study revealed that ANC, ALC, the presence of hydrocephalus, GCS score at admission, and hematoma volume all had an independent relationship with admission NLR in intracerebral hemorrhage [33]. In this regard, logistic regression is used to assess the probabilities of an outcome while controlling for certain clinical variables. Our multivariable analysis indicated links between NLR, age, and level of consciousness with the mortality rate. In an adjusted multivariate logistic regression model, only the level of consciousness remained statistically significant after accounting for these unique variables. These findings support the concept that hydrocephalus is a complex disease. Although a causative association cannot be shown in this research, some of these parameters appear to be relevant to the progression of acute hydrocephalus. The relationship between these measures, independent of the exact etiopathogenesis, provides clinically relevant details for the management of hydrocephalus after EVD. Following that, we discovered that having an NLR>8.88 with a GCS score <8 (coma and semicoma) was associated with higher mortality and a worse prognosis after EVD in hydrophilic patients. Other studies revealed the same finding; however, many of them did not show that the treatment approach affected the outcome. According to one study, individuals who had intracranial aneurysms and an increased NLR on admission had a greater in-hospital mortality rate, although there were inadequate statistical measures to control for relevant variables [34]. A further investigation discovered that NLR can be used as an independent biomarker to predict clinical results following aneurysm rupture. However, age was not included in the multivariate regression model [35]. Menon et al. conducted a similar investigation. In this work, the NLR was investigated as a new prognostic predictor following intracerebral hemorrhage. Higher NLR on admission was independently connected to death and 90-day prognosis following intracerebral hemorrhage [36]. Wang et al. discovered a link between NLR levels and 30-day mortality by observing that patients who died the next day after admission had considerably greater NLR than survivors [37]. They suggested 7.35 as the best NLR threshold value for distinguishing survivors from non-survivors and confirmed their findings in a second study, which determined NLR>7.35 to be a credible indicator of worse short-term prognosis. Wang et al. in another study found that the increasing trend of NLR over one week was an additional independent indicator of death [38]. According to Gökhan et al. admission NLR values in dead subjects with acute cerebrovascular episodes were considerably greater than in survivors [39]. Furthermore, a cohort revealed that the mean NLR in those who worsened was considerably greater, and the optimum threshold NLR in the study was 8.2 [36]. Our findings also support an association between NLR>8.88 paired with a GCS score <8 and a poor prognosis of hydrocephalus after EVD. This could be useful in assessing the outcomes of hydrophilic individuals treated with EVD in clinical settings. However, more research is needed to determine whether close monitoring of certain subsets of patients with hydrocephalus who have higher NLR can result in better outcome measures.
5. Conclusion
Admission NLR is a simple, inexpensive, and accurate predictor of outcomes following EVD in hydrocephalus patients. A high CSF NLR is related to an increased possibility of death and an unfavorable outcome. Admission NLR>8.88 considerably enhances predicting results after EVD when combined with a GSC score <8. More investigation is required to determine the precise processes by which CSF indicators, in conjunction with NLR, affect the prognosis of hydrocephalus patients following EVD.
Limitations
This study faced some limitations that should be addressed when interpreting the results. First, because this was a retrospective, single-center study, systematic bias was unavoidable. Second, this study did not examine additional inflammation-related biomarkers like C-reactive protein and interleukin-6. As a result, while multivariable logistic analysis was used to adjust for the confounding parameters, undetected factors may also have an impact on our final results. Third, due to the restrictions of retrospective data, we were unable to investigate the dynamic NLR, which may have resulted in inevitable bias. More studies with bigger samples may be required to find meaningful effects of dynamic changes in the NLR on the outcomes of hydrocephalus patients. Serial trends in NLR may also be a stronger predictor of outcome than a single independent score on admission. Our study demonstrated useful information on the predictive efficacy of NLR as a low-cost approach, which may lead to additional research in this field.
Ethical Considerations
Compliance with ethical guidelines
There were no ethical considerations to be considered in this research.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interpretation of the results, and drafting of the manuscript. Each author approved the final version of the manuscript for submission.
Conflict of interest
The authors declare no conflict of interest.
References
Hydrocephalus is the leading cause of neurosurgical conditions globally, which involves the expansion of the brain ventricles filled with cerebrospinal fluid (CSF) as a result of impaired CSF homeostasis, culminating in progressive dilation of the brain ventricular system [1]. Regardless of the cause, hydrocephalus is frequently defined by elevated intracranial pressure, enlarged ventricular chambers from CSF accumulation, and brain structural damage, which can lead to neurological deterioration, coma, and death if not treated [2]. When hydrocephalus is diagnosed, CSF diversion is required to keep normal cerebral pressure. The insertion of an external ventricular drain (EVD) is the initial therapy for acute hydrocephalus, allowing for the diversion and control of excess CSF, dependent on the total drainage status, to mitigate the related rise in intracranial pressure, which, if left untreated, may contribute to lower brain circulation and later neurological impairment [3].
Several studies have found brain and CSF inflammation after EVD treatment in both posthemorrhagic and postinfectious hydrocephalus [4]. Although the restoration of inflammatory responses is critical for the removal of invading pathogens, damaged cells, and irritating substances, it can also develop or promote the disease if it is incorrectly induced or prolonged. The presence of multiple inflammatory agents in the circulatory system or CSF has been linked to an increased risk for post-hemorrhagic or post-infectious hydrocephalus, as well as a greater degree of symptoms [5]. There is accumulating evidence that an immune-related inflammation in the central nervous system (CNS) is a major cause of initial posttraumatic cerebral damage and related clinical outcomes [6]. According to experimental and clinical research, EVD activates and proliferates several leukocyte subtypes (e.g. neutrophils, lymphocytes) in mouse models and humans with hydrocephalus [7, 8]. High neutrophil counts stimulate the neuro-inflammation pathway, exacerbating edema and hematoma formation, increasing mass impact and intracranial pressure, and resulting in nervous system impairment [9]. Lymphocytes, as an adaptive immune response, are necessary for bodily defense, and low lymphocyte counts imply a worse prognosis in hydrocephalus patients with an increased incidence of infections [10].
The neutrophil-to-lymphocyte ratio (NLR) has been suggested as a valid compound indicator and dynamic scale of the inflammatory process by calculating total neutrophil and lymphocyte numbers [11]. The NLR represents the immune response and integrates data from both the innate and adaptive. In addition, since counts of neutrophils and lymphocytes are frequently evaluated during laboratory tests, the NLR is useful in clinical settings. NLR has been widely studied and found to be linked with consequences, with high NLR having prognostic value for numerous disorders, such as cardiovascular disease [12], ischemic stroke [13], cerebral hemorrhage [14], and infectious diseases [15]. Furthermore, greater NLR is linked to a worse prognosis in cancer patients [16]. These negative connections could be related to the roles of excessive inflammation and impaired immunological activity in the course of these disorders. As a result, NLR is a helpful indicator of vulnerability to subsequent brain injury and post-stroke problems caused by increased neutrophils and decreased lymphocytes [17]. There is evidence that patients with higher neutrophil levels and lower lymphocyte levels had less favorable outcomes in ischemic and hemorrhagic strokes [18]. These results suggest that assessing the NLR in the CSF of patients with hydrocephalus may be especially important because inflammatory responses emerge to have a substantial impact on prognosis following EVD treatment. NLR may thus be predictive of death in hydrocephalus patients, as well as the general influence of inflammation and the immune system on health. A better understanding of the relationship between NLR and critical clinical factors on mortality rate would assist in elucidating the function of inflammation and immune response in the progression and consequences of many diseases. While several studies have examined the predictive usefulness of NLR in terms of mortality rates because of cancer, cardiac disease, or stroke, no research has examined such relationships in the context of hydrocephalus. The present study examines the connections of the NLR combined with significant clinical parameters with overall mortality and prognosis in the CSF of patients with hydrocephalus after EVD to provide more support information for hydrocephalus management.
2. Methods and Materials/Patients
Study design
We conducted a cross-sectional study on 40 consecutive hydrocephalus patients who underwent EVD insertions in the Neurosurgery Ward of Poursina Hospital in Rasht City, Iran, January 2020 and December 2022. The Ethics Committee of the hospital approved the study design. All patients or their families provided informed consent. In addition, a convenient means of sampling was selected in this research.
Patient selection
The inclusion criteria were as follows: 1) all patients with hydrocephalus on admission computed tomography (CT) who had EVD insertion and a CSF sample taken from the surgical site; 2) patient age ≥18 years; 3) the duration of intensive care unit (ICU) and hospitalization, as well as short-term mortality (death occurred before hospital discharge) were recorded; 4) first CSF specimen for laboratory tests 24 h after admission; 5) white blood cell count greater than 5 in CSF sample and cell index greater than 1 in case of intraventricular hemorrhage(IVH).
In addition, the exclusion crieteria included the following items: 1) the lack of laboratory results for testing 24 h after admission; 2) <4 days survival from the onset of symptoms; 3) individuals who had surgery before the 24-h CT; 4) past cerebral abnormalities such as ischemia or hemorrhagic stroke; 5) immunodeficiency or autoimmune disorders; 6) hematologic diseases and tumors; 7) a history of systemic problems, such as uremia, liver cirrhosis, chronic heart or lung disease; 8) patients who met the inclusion criteria but had insufficient data on their charts. Medical records were used to obtain clinical data and imaging scans for each patient, and an online pathology registry was used to collect microbiology and biochemistry reports. The data from the patients were then retrospectively analyzed, and a variety of parameters (detailed in the following sections) were evaluated.
EVD indications
The EVD was inserted on the clinically preferred side. The clinical indication determined the EVD height, which was opened to drainage when the intracranial pressure exceeded a threshold of 20 mmHg. Clinical manifestations (such as mental status changes, lethargy, somnolence, or pupillary alterations) and radiographic data indicating acute hydrocephalus (such as ventriculomegaly, increase in temporal horn size, cisternal effacement, or sulcal effacement) were both considered when deciding whether or not to insert an EVD at the time of admission. Lumbar drains were not employed to divert CSF.
Parameters in clinical and laboratory settings
Patients were divided into two groups: Subjects who were alive (n=20) and subjects who were dead (n=20). We analyzed demographic data (age, gender), clinical status (level of consciousness, underlying disease, type of primary disease, and history of COVID-19 and organ failure), and laboratory data (neutrophil, lymphocyte, and NLR) collected from CSF 24 h after admission. An autoanalyzer was used to measure the number of white blood cells, neutrophils, and lymphocytes. Our hospital laboratory equipment was used to conduct an absolute neutrophil count (ANC) and absolute lymphocyte count (ALC). NLR was then determined using the ANC/ALC methodology.
Statistical analysis
The demographic data is demonstrated in a table format, with numerical parameters using the Mean±SD and categorical factors using numbers and percentages. The Fisher exact test for proportions, the Student t-test for continuous normally distributed data, and the Mann-Whitney test for non-normally distributed continuous data were used for comparing baseline features in those who had or did not have an event of death before discharge. To generate the clinical significance of an odds ratio (OR) with 95% confidence intervals (CI), outcome factors were examined using adjusted and unadjusted data in simple and multiple logistic regression models. Multiple logistic regression models were employed to examine the relationship between mortality and clinically significant prognostic markers, such as age, underlying disease, level of consciousness, and NLR. To demonstrate the predictive properties of various laboratory measurements related to mortality, receiver operating characteristic (ROC) curves were designed. The Binomial exact method was used to investigate the risk of mortality related to critical parameters and calculate the CI for the area under the curve (AUC). Furthermore, the DeLong et al. test was employed to determine the statistically significant variations between curves. Meanwhile, P<0.05 were used to determine statistical significance. All statistical analyses were carried out using IBM SPSS software, version 21.0, MedCalc software, version 20.026, and GraphPad Prism software, version 9.0.0.
3. Results
We examined patient database entries from 2020 to 2022. A total of 40 patients with hydrocephalus who were treated surgically with EVD insertion for CSF diversion on admission and met the inclusion criteria were found, for whom follow-up data were available. The baseline demographic and clinical characteristics of patients diagnosed with acute symptomatic hydrocephalus are summarized in Table 1. As previously stated, the patients were separated into two groups: Dead (n=20) and alive (n=20). All patients were adults, with mean ages ranging from 22 to 78 years (51.68±16.34; P=0.038), and there were more males in the population (60%). Median glasgow coma score (GCS) on admission ranged from 3 to 13, with a Mean±SD of 7.10±2.39, and 24 patients (60%) presented with a GCS<8. The median presentation GCS in alive patients was 8.85 (6-13) in comparison to 5.35 (3-8) in dead patients (P≤0.001). The median duration of ICU admission was 6.5 days, and that of overall hospital stay was 14 days; days with an EVD were not different between groups. Overall, mortality was 20 from 40 cases (50%). More than half of the patients had an intracranial hemorrhage (55%), whereas about a fifth had no history of COVID-19 or organ failure and underlying disease (82.5% and 80%, respectively). The mean NLR in our entire study was 6.77±5.55. Patients who died showed greater NLRs than those who were alive, with median NLRs of 8.49 vs 5.05, respectively (P=0.027).
ROC curve
To assess the predictive potential of the selected indicators, ROC curves were provided. Actual NLR results on the value of markers on admission for hydrocephalus indicated an appropriate AUC (AUC=0.702, 95% CI, 0.537 %, 0.836%; P=0.0171; Figure 1). The optimal NLR threshold value for predicting mortality rate was 8.88 with a sensitivity and specificity of 40% and 100%, respectively. In addition, the actual values of underlying disease (AUC=0.650; 95% CI, 0.483%, 0.794%; P=0.0126), consciousness level (AUC=0.946; 95% CI, 0.825%, 0.993%; P<0001), and age (AUC=0.674; 95% CI, 0.507%, 0.813%; P=0.0496) potentially predict mortality, while classified values of other clinical factors appear to be poor predictors (Figure 1). Table 2 analyzes the relationship between NLR and important factors in both patient groups who died and those who did not survive. The correlation of NLR with the level of consciousness was statistically significant (CI, 0.0761%, 0.411%; P=0.0044). In contrast, there was no significant difference in patients with NLR related to age and underlying disease.
NLR correlation with factors predicting mortality and clinical prognosis
To further analyze the effect of NLR on mortality, the dead group was divided based on age, GCS, and underlying disease. As shown in Figure 2, mortality in patients with an admission GCS<8 was 90% (18/20) and was statistically greater than in those with a GCS>8. The level of consciousness varied from coma (n=4), semicoma (n=14), and stupor (n=2). The GCS scores of coma, semicoma, and stupor were 3.5±0.28, 5.66±0.21, and 8.5±0.5, respectively (Figure 2). The GCS scores did not differ significantly between coma and semicoma levels. GCS scores also increased as the consciousness level increased. NLR was significantly different in the three groups by GCS in coma and semicoma groups compared to the stupor group (P<0.05). Univariate analysis revealed that NLR in age and underlying disease was not significantly correlated with mortality.
Logistic regression
Logistic regression analysis was used to predict unfavorable results using significant univariate characteristics (Table 3). The level of consciousness on admission was associated with mortality (OR=0.23; 95% CI, 0.08 %, 0.65%; P=0.005). According to these regression analyses, there were no significant indicators for sex, age, or overall NLR. We then characterized dead patients based on the rate of NLR (>8.88 vs <8.88) in the CSF. A total of 10 (50%) patients had an NLR<8.88, and 50(50%) >8.88 (P<0.0001; Figure 3). The median GCS in individuals with NLR<8.88 was 5.88, compared to 4.58 in those with NLR>8.88. In addition, the number of patients with GCS<8 was higher than the GCS<8 group. The NLR>8.88 group had a greater mortality rate in terms of coma (30%) and semicoma (70%) (P<0.0001; Table 4).
4. Discussion
To the best of the authors’ knowledge, this is the first study to investigate the connections between high NLR and GSC scores in the CSF of hydrocephalus patients following EVD. In this study, we discovered that a higher NLR combined with GSC score was substantially linked with death, implying that neutrophils and lymphocytes may play a role in the poor prognosis. In the first step, we identified many risk variables for acute symptomatic hydrocephalus after EVD. According to our univariate analysis, the affected patients had a mean age of 51.6 years, with 60% being men. The average age and gender of patients can be important determinants of mortality. According to the findings, comparing the average ages of patients with mortality and surviving patients revealed a significant difference (P=0.038), and the average age of patients with mortality was higher. At older ages, the increase in the probability of mortality in men appears to be inversely proportional to the increase in the probability of discharge, implying that men die more frequently in hospitals [19]. We examined several of these cases, which included primary disease, a history of COVID-19 infection, and organ failure. The findings revealed that more than 80% of the patients did not report a history of organ failure or even the COVID-19 virus. To some extent, these circumstances can mitigate the disturbing effect of organ failure on patient mortality. Furthermore, there was no significant difference in gender between those who died and those who were alive. A similar study found that the general connection between age and premature death is similar in men and women. James et al. examined the relationship between the age and gender of people with cerebral hemorrhage and concluded that as men and women age, the rate of in-hospital death increases slightly more in men than in women [20].
We also discovered that the average level of consciousness in patients who died was lower than in those who were alive (P<0.001). The GCS was the initial objective scoring index used to evaluate patients’ levels of consciousness. According to Teasdale et al. there was a link between GCS score measurement and clinical outcomes, demonstrating a link between a drop in GCS score and an increase in mortality [21]. A low GCS score is an independent predictor of poor prognosis in hemodialysis patients with subarachnoid hemorrhage and traumatic intracranial hemorrhage [22-24]. The GCS score can independently predict hospital mortality; nonetheless, GCS has limitations as a subjective rating tool. For instance, measuring the GCS score in individuals who are sedated, on a ventilator, have jaw and face trauma, or are under the influence of illegal substances or alcohol is problematic [25].
NLR is a biomarker that indicates the equilibrium of the two components of the immune system. It is determined as a simple ratio of the count of neutrophils to lymphocytes in the circulatory system. This ratio is also computed in the CSF. NLR may be a predictor of overall population mortality, as well as the impact of inflammation and immunology on health [26]. Our findings revealed that the average NLR in patients who died was considerably higher than in survivors (P=0.027). The first indication of cerebral hemorrhage is blood flow stagnation, which can be detected both within and surrounding the hematoma. Following that, the blood-brain barrier is disrupted. Endothelial cells, as well as dying neurons and glial cells, release a large number of inflammatory molecules [27, 28]. The first inflammatory cells to enter the site are neutrophils, followed by the activation of lymphocytes as adaptive immune system cells [29]. Therefore, a deeper knowledge of the association between NLR or other clinical indicators and overall mortality in the CSF provides insight into the function of inflammation and immunity in disease development and prognosis. NLR could be used to track patients who have undergone EVD and predict their prognosis and mortality [30]. As a result, we investigated the likelihood of using the biomarkers independent of the thresholds reported in the study. For this purpose, regression analysis as well as ROC curves were used. The ROC curve contrasts the ability of a true-positive rate (sensitivity) and a false-positive rate (specificity) to predict a dichotomous result over a range of values. In our findings, the levels of age, NLR, underlying disease, and level of consciousness were associated with the mortality rate and, as continuous factors, indicated a better AUC. Several studies have been conducted to evaluate the NLR function as a predicted inflammatory biomarker in the mortality rate after EVD [30-32]. Our study was the first to investigate the major characteristics linked with NLR for death rate in patients with hydrocephalus. The present findings revealed that the connection between NLR and the level of consciousness (coma vs stupor group) was much higher in the dead group. A retrospective cohort study revealed that ANC, ALC, the presence of hydrocephalus, GCS score at admission, and hematoma volume all had an independent relationship with admission NLR in intracerebral hemorrhage [33]. In this regard, logistic regression is used to assess the probabilities of an outcome while controlling for certain clinical variables. Our multivariable analysis indicated links between NLR, age, and level of consciousness with the mortality rate. In an adjusted multivariate logistic regression model, only the level of consciousness remained statistically significant after accounting for these unique variables. These findings support the concept that hydrocephalus is a complex disease. Although a causative association cannot be shown in this research, some of these parameters appear to be relevant to the progression of acute hydrocephalus. The relationship between these measures, independent of the exact etiopathogenesis, provides clinically relevant details for the management of hydrocephalus after EVD. Following that, we discovered that having an NLR>8.88 with a GCS score <8 (coma and semicoma) was associated with higher mortality and a worse prognosis after EVD in hydrophilic patients. Other studies revealed the same finding; however, many of them did not show that the treatment approach affected the outcome. According to one study, individuals who had intracranial aneurysms and an increased NLR on admission had a greater in-hospital mortality rate, although there were inadequate statistical measures to control for relevant variables [34]. A further investigation discovered that NLR can be used as an independent biomarker to predict clinical results following aneurysm rupture. However, age was not included in the multivariate regression model [35]. Menon et al. conducted a similar investigation. In this work, the NLR was investigated as a new prognostic predictor following intracerebral hemorrhage. Higher NLR on admission was independently connected to death and 90-day prognosis following intracerebral hemorrhage [36]. Wang et al. discovered a link between NLR levels and 30-day mortality by observing that patients who died the next day after admission had considerably greater NLR than survivors [37]. They suggested 7.35 as the best NLR threshold value for distinguishing survivors from non-survivors and confirmed their findings in a second study, which determined NLR>7.35 to be a credible indicator of worse short-term prognosis. Wang et al. in another study found that the increasing trend of NLR over one week was an additional independent indicator of death [38]. According to Gökhan et al. admission NLR values in dead subjects with acute cerebrovascular episodes were considerably greater than in survivors [39]. Furthermore, a cohort revealed that the mean NLR in those who worsened was considerably greater, and the optimum threshold NLR in the study was 8.2 [36]. Our findings also support an association between NLR>8.88 paired with a GCS score <8 and a poor prognosis of hydrocephalus after EVD. This could be useful in assessing the outcomes of hydrophilic individuals treated with EVD in clinical settings. However, more research is needed to determine whether close monitoring of certain subsets of patients with hydrocephalus who have higher NLR can result in better outcome measures.
5. Conclusion
Admission NLR is a simple, inexpensive, and accurate predictor of outcomes following EVD in hydrocephalus patients. A high CSF NLR is related to an increased possibility of death and an unfavorable outcome. Admission NLR>8.88 considerably enhances predicting results after EVD when combined with a GSC score <8. More investigation is required to determine the precise processes by which CSF indicators, in conjunction with NLR, affect the prognosis of hydrocephalus patients following EVD.
Limitations
This study faced some limitations that should be addressed when interpreting the results. First, because this was a retrospective, single-center study, systematic bias was unavoidable. Second, this study did not examine additional inflammation-related biomarkers like C-reactive protein and interleukin-6. As a result, while multivariable logistic analysis was used to adjust for the confounding parameters, undetected factors may also have an impact on our final results. Third, due to the restrictions of retrospective data, we were unable to investigate the dynamic NLR, which may have resulted in inevitable bias. More studies with bigger samples may be required to find meaningful effects of dynamic changes in the NLR on the outcomes of hydrocephalus patients. Serial trends in NLR may also be a stronger predictor of outcome than a single independent score on admission. Our study demonstrated useful information on the predictive efficacy of NLR as a low-cost approach, which may lead to additional research in this field.
Ethical Considerations
Compliance with ethical guidelines
There were no ethical considerations to be considered in this research.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interpretation of the results, and drafting of the manuscript. Each author approved the final version of the manuscript for submission.
Conflict of interest
The authors declare no conflict of interest.
References
- Duy PQ, Rakic P, Alper SL, Robert SM, Kundishora AJ, Butler WE, et al. A neural stem cell paradigm of pediatric hydrocephalus. Cerebral Cortex. 2023; 33(8):4262-79. [DOI:10.1093/cercor/bhac341] [PMID]
- Juhler M. Hydrocephalus. In: Praetorius J, Blazer-Yost B, Damkier H, editors. Role of the choroid plexus in health and disease. Berlin: Springer; 2020. [DOI:10.1007/978-1-0716-0536-3_12]
- Capion T, Lilja-Cyron A, Olsen MH, Juhler M, Møller K, Sorteberg A, et al. Prompt closure versus gradual weaning of external ventricular drainage for hydrocephalus following aneurysmal subarachnoid haemorrhage: Protocol for the DRAIN randomised clinical trial. Acta Anaesthesiologica Scandinavica. 2023 [Unpublished]. [DOI:10.21203/rs.3.rs-3136591/v1]
- Gaderer C, Schaumann A, Schulz M, Thomale UW. Neuroendoscopic lavage for the treatment of CSF infection with hydrocephalus in children. Child'S Nervous System. 2018; 34(10):1893-903. [DOI:10.1007/s00381-018-3894-7] [PMID]
- Robert SM, Reeves BC, Kiziltug E, Duy PQ, Karimy JK, Mansuri MS, et al. The choroid plexus links innate immunity to CSF dysregulation in hydrocephalus. Cell. 2023; 186(4):764-85.e21. [DOI:10.1016/j.cell.2023.01.017] [PMID]
- Risbrough VB, Vaughn MN, Friend SF. Role of inflammation in traumatic brain injury-associated risk for neuropsychiatric disorders: State of the evidence and where do we go from here. Biological Psychiatry. 2022; 91(5):438-48. [DOI:10.1016/j.biopsych.2021.11.012] [PMID]
- Cuoco JA, Guilliams EL, Klein BJ, Witcher MR, Marvin EA, Patel BM, et al. Monocyte count on admission is predictive of shunt-dependent hydrocephalus after aneurysmal subarachnoid hemorrhage. Frontiers in Surgery. 2022; 9:879050. [DOI:10.3389/fsurg.2022.879050] [PMID]
- Cuoco JA, Guilliams EL, Klein BJ, Benko MJ, Darden JA, Olasunkanmi AL, et al. Neutrophil count on admission predicts acute symptomatic hydrocephalus after aneurysmal subarachnoid hemorrhage. World Neurosurgery. 2021; 156:e338-44. [DOI:10.1016/j.wneu.2021.09.059] [PMID]
- Zhao H, Li Y, Zhang Y, He WY, Jin WN. Role of immune and inflammatory mechanisms in stroke: A review of current advances. Neuroimmunomodulation. 2022; 29(4):255-68. [DOI:10.1159/000524951]
- Liu L, Zhang R, Tang Y, Lu H. The use of ventriculoperitoneal shunts for uncontrollable intracranial hypertension in patients with HIV-associated cryptococcal meningitis with or without hydrocephalus. Bioscience Trends. 2014; 8(6):327-32.[DOI:10.5582/bst.2014.01070] [PMID]
- Piri Cinar B, Kunt R, Yuksel B, Gulluoglu H, Sayilir I, Celiker Uslu S, et al. Assessment of the relation between the neutrophil to lymphocyte ratio and severity of ischemic stroke in a large cohort. International Journal of Clinical Practice. 2021; 75(4):e13955. [DOI:10.1111/ijcp.13955] [PMID]
- Han K, Shi D, Yang L, Wang Z, Li Y, Gao F, et al. Prognostic value of systemic inflammatory response index in patients with acute coronary syndrome undergoing percutaneous coronary intervention. Annals of Medicine. 2022; 54(1):1667-77. [DOI:10.1080/07853890.2022.2083671] [PMID]
- Hu X, Liang J, Hao W, Zhou J, Gao Y, Gong X, et al. Prognostic value of inflammatory markers for in-hospital mortality in intensive care patients with acute ischemic stroke: A retrospective observational study based on MIMIC-IV. Frontiers in Neurology. 2023; 14:1174711. [DOI:10.3389/fneur.2023.1174711] [PMID]
- Tao C, Hu X, Wang J, Ma J, Li H, You C. Admission neutrophil count and neutrophil to lymphocyte ratio predict 90-day outcome in intracerebral hemorrhage. Biomarkers in Medicine. 2017; 11(1):33-42. [DOI:10.2217/bmm-2016-0187] [PMID]
- Li T, Dong G, Zhang M, Xu Z, Hu Y, Xie B, et al. Association of neutrophil-lymphocyte ratio and the presence of neonatal sepsis. Journal of Immunology Research. 2020; 2020:7650713. [DOI:10.1155/2020/7650713] [PMID]
- Van Berckelaer C, Van Geyt M, Linders S, Rypens C, Trinh X, Tjalma W, et al. A high neutrophil-lymphocyte ratio and platelet-lymphocyte ratio are associated with a worse outcome in inflammatory breast cancer. The Breast. 2020; 53:212-20. [DOI:10.1016/j.breast.2020.08.006] [PMID]
- Yu S, Arima H, Bertmar C, Clarke S, Herkes G, Krause M. Neutrophil to lymphocyte ratio and early clinical outcomes in patients with acute ischemic stroke. Journal of the Neurological Sciences. 2018; 387:115-8. [DOI:10.1016/j.jns.2018.02.002] [PMID]
- Dehghanei M, ArefNezhad R, Motedayyen H. The predicting role of neutrophil–lymphocyte ratio in patients with acute ischemic and hemorrhagic stroke. Journal of Stroke and Cerebrovascular Diseases. 2020; 29(11):105233. [DOI:10.1016/j.jstrokecerebrovasdis.2020.105233] [PMID]
- Goldstein R, Cotten C, Shankaran S, Gantz M, Poole W. Influence of gestational age on death and neurodevelopmental outcome in premature infants with severe intracranial hemorrhage. Journal of Perinatology. 2013; 33(1):25-32. [DOI:10.1038/jp.2012.91] [PMID]
- Simon T, Mary-Krause M, Cambou JP, Hanania G, Guéret P, Lablanche JM, et al. Impact of age and gender on in-hospital and late mortality after acute myocardial infarction: increased early risk in younger women: Results from the French nation-wide USIC registries. European Heart Journal. 2006; 27(11):1282-8. [DOI:10.1093/eurheartj/ehi719] [PMID]
- Teasdale G, Jennett B. Assessment of coma and impaired consciousness. A practical scale. Lancet. 1974; 2(7872):81-4. [DOI:10.1016/S0140-6736(74)91639-0] [PMID]
- Huang BR, Liao CC, Huang WH, Hsu YH, Hsu JC, Yen HC, et al. Prognostic factors of spontaneous intracerebral haemorrhage in haemodialysis patients and predictors of 30-day mortality. Internal Medicine Journal. 2008; 38(7):568-74. [DOI:10.1111/j.1445-5994.2007.01536.x] [PMID]
- Oishi T, Takehara S, Yamamura Y, Tomida M, Ikegaya N, Seki G, et al. Hemodialysis increases the incidence of post-traumatic seizure in hemodialysis patients with traumatic intracranial hemorrhage. No Shinkei geka. Neurological Surgery. 2017; 45(4):303-9. [DOI:10.11477/mf.1436203500] [PMID]
- Yousefzadeh-Chabok S, Kazemnejad-Leili E, Kouchakinejad-Eramsadati L, Hosseinpour M, Ranjbar F, Malekpouri R, et al. Comparing Pediatric Trauma, Glasgow Coma Scale and Injury Severity scores for mortality prediction in traumatic children. Turkish Journal of Trauma and Emergency Surgery. 2016; 22(4):328-32. [DOI:10.5505/tjtes.2015.83930] [PMID]
- Meredith W, Rutledge R, Fakhry SM, Emery S, Kromhout-Schiro S. The conundrum of the Glasgow coma scale in intubated patients: A linear regression prediction of the Glasgow verbal score from the Glasgow eye and motor scores. Journal of Trauma and Acute Care Surgery. 1998; 44(5):839-45. [DOI:10.1097/00005373-199805000-00016] [PMID]
- Song M, Graubard BI, Rabkin CS, Engels EA. Neutrophil-to-lymphocyte ratio and mortality in the United States general population. Scientific Reports. 2021; 11(1):464. [DOI:10.1038/s41598-020-79431-7] [PMID]
- Aronowski J, Zhao X. Molecular pathophysiology of cerebral hemorrhage: secondary brain injury. Stroke. 2011; 42(6):1781-6. [DOI:10.1161/STROKEAHA.110.596718] [PMID]
- Anrather J, Iadecola C. Inflammation and Stroke: An Overview. Neurotherapeutics. 2016; 13(4):661-70. [DOI:10.1007/s13311-016-0483-x] [PMID]
- Merali Z, Huang K, Mikulis D, Silver F, Kassner A. Evolution of blood-brain-barrier permeability after acute ischemic stroke. Plos One. 2017; 12(2):e0171558. [DOI:10.1371/journal.pone.0171558] [PMID]
- Gusdon AM, Thompson CB, Quirk K, Mayasi YM, Avadhani R, Awad IA, et al. CSF and serum inflammatory response and association with outcomes in spontaneous intracerebral hemorrhage with intraventricular extension: An analysis of the CLEAR-III Trial. Journal of Neuroinflammation. 2021; 18(1):1-11. [DOI:10.1186/s12974-021-02224-w] [PMID]
- Kaleem S, Zhang C, Gusdon AM, Oh S, Merkler AE, Avadhani R, et al. Association between neutrophil–lymphocyte ratio and 30-day infection and thrombotic outcomes after intraventricular hemorrhage: A clear III analysis. Neurocritical care. 2024; 40(2):529-37. [DOI:10.1161/str.54.suppl_1.TP121]
- Hirsch Y, Geraghty JR, Katz EA, Testai FD. Inflammasome caspase-1 activity is elevated in cerebrospinal fluid after aneurysmal subarachnoid hemorrhage and predicts functional outcome. Neurocritical Care. 2021; 34(3):889-98. [DOI:10.1007/s12028-020-01113-z] [PMID]
- Zhang F, Tao C, Hu X, Qian J, Li X, You C, et al. Association of neutrophil to lymphocyte ratio on 90-day functional outcome in patients with intracerebral hemorrhage undergoing surgical treatment. World Neurosurgery. 2018; 119:e956-61. [DOI:10.1016/j.wneu.2018.08.010] [PMID]
- Zhang B, Lin L, Yuan F, Song G, Chang Q, Wu Z, et al. Clinical application values of neutrophil-to-lymphocyte ratio in intracranial aneurysms. Aging. 2021; 13(4):5250. [DOI:10.18632/aging.202445] [PMID]
- Tao C, Wang J, Hu X, Ma J, Li H, You C. Clinical value of neutrophil to lymphocyte and platelet to lymphocyte ratio after aneurysmal subarachnoid hemorrhage. Neurocritical Care. 2017; 26(3):393-401. [DOI:10.1007/s12028-016-0332-0] [PMID]
- Menon G, Johnson SE, Hegde A, Rathod S, Nayak R, Nair R. Neutrophil to lymphocyte ratio - A novel prognostic marker following spontaneous intracerebral haemorrhage. Clinical Neurology and Neurosurgery. 2021; 200:106339. [DOI:10.1016/j.clineuro.2020.106339] [PMID]
- Wang F, Hu S, Ding Y, Ju X, Wang L, Lu Q, et al. Neutrophil-to-lymphocyte ratio and 30-day mortality in patients with acute intracerebral hemorrhage. Journal of Stroke and Cerebrovascular Diseases. 2016; 25(1):182-7. [DOI:10.1016/j.jstrokecerebrovasdis.2015.09.013] [PMID]
- Wang F, Wang L, Jiang TT, Xia JJ, Xu F, Shen LJ, et al. Neutrophil-to-lymphocyte ratio is an independent predictor of 30-day mortality of intracerebral hemorrhage patients: A validation cohort study. Neurotoxicity Research. 2018; 34(3):347-52. [DOI:10.1007/s12640-018-9890-6] [PMID]
- Gökhan S, Ozhasenekler A, Durgun HM, Akil E, Ustündag M, Orak M. Neutrophil lymphocyte ratios in stroke subtypes and transient ischemic attack. Age. 2013; 17: 653-7. [Link]
Type of Study: Research |
Subject:
Basic Neurosurgery
| Rights and Permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
