Mon, Jul 6, 2026
Volume 11 - Continuous Publishing
Iran J Neurosurg 2025, 11 - Continuous Publishing: 0-0 |
Back to browse issues page
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Batiar A, Mirbolouk M H, Nabiuni M, Fateme A, Shahrokhi F, Kohansal R et al . Endovascular Coiling Versus Neurosurgical Clipping for Aneurysmal Subarachnoid Hemorrhage: Single-center Experience. Iran J Neurosurg 2025; 11 : 11
URL: http://irjns.org/article-1-451-en.html
URL: http://irjns.org/article-1-451-en.html
Ali Batiar1 
 , Mohammad Hossein Mirbolouk2 , Mohsen Nabiuni2 , Aidin Fateme1 , Fateme Shahrokhi1 , Rahim Kohansal1 , Rouzbeh Shams Amiri *3
, Mohammad Hossein Mirbolouk2 , Mohsen Nabiuni2 , Aidin Fateme1 , Fateme Shahrokhi1 , Rahim Kohansal1 , Rouzbeh Shams Amiri *3
, Mohammad Hossein Mirbolouk2 , Mohsen Nabiuni2 , Aidin Fateme1 , Fateme Shahrokhi1 , Rahim Kohansal1 , Rouzbeh Shams Amiri *3
1- Golestan University of medical sciences
2- Iran University of Medical Science
3- Golestan University of medical sciences ,rshamsa@gmail.com
2- Iran University of Medical Science
3- Golestan University of medical sciences ,
Full Text [PDF 873 kb]
(373 Downloads)
| Abstract (HTML) (853 Views)
Full Text: (242 Views)
1. Introduction
Subarachnoid hemorrhage (SAH) due to aneurysmal rupture is a relatively common disease with a reported prevalence of 10 to 15 people per 100000 population in the USA [1]. Aneurysmal SAH is related to 30-day mortality rates of 80% to 100% compared to 33% to 50% in SAH overall [2]. This life-threatening condition is commonly diagnosed with a non-contrast brain computed tomography scan with or without diagnostic lumbar puncture [3]. Interventions are primarily trying to resuscitate the patient and reduce dependence in survivors. There are two common methods used for the treatment of SAH, trying to reduce rebleeding after SAH, including surgical clipping and endovascular coiling [4].
The gold standard intervention for SAH treatment is neurosurgical clipping [5]. This method is performed by clipping the aneurysm using a titanium clip and through access using a large craniotomy. Neurosurgical clipping results in an extended recovery time and is related to an increased risk of complications [5]. Minimally invasive methods, such as endovascular coiling, have been developed with advancements in interventional neuroradiology as an alternative treatment for aneurysmal SAH [6]. In this method, a platinum coil is attached to a microcatheter tip, which delivers it to the aneurysm lumen. Then, the coil is detached from the microcatheter, resulting in intra-aneurysmal thrombosis and its closure. Some studies suggest that the independence rate is higher in patients who were treated using endovascular coiling compared to neurosurgical clipping, with an increased risk of rebleeding in the coiling method [7]. However, there are contradictory results demonstrated by other studies regarding outcomes and complications [5].
There is a controversy between the studies regarding the efficacy and complications of each approach. Furthermore, these results could vary a lot in different settings and populations. To the best of our knowledge, no published investigation has been conducted comparing neurosurgical clipping and endovascular coiling in Iran. Therefore, this study compares these two conventional methods for aneurysmal SAH in our center with a focus on functional outcomes.
2. Materials and Methods
Study design and setting
This was a retrospective cohort study performed on consecutive patients with aneurysmal SAH who underwent either neurosurgical clipping or endovascular coiling at the Sayad-Shirazi or 5-Azar hospitals (both affiliated with Golestan University of Medical Sciences). The patients were referred for surgery from November 2016 to March 2021 and were followed up for two years. The medical records of each patient were extracted and were later used for comparison between the two approaches. This cohort was conducted adhering to the Declaration of Helsinki and its later amendments. We report the study based on strengthening the reporting of observational studies in epidemiology criteria for cohort studies.
Study participants
All patients afflicted with aneurysmal SAH who were referred to our two hospitals and were treated with either neurosurgical clipping or endovascular coiling were included in this cohort. The exclusion criteria were as follows: a) non-aneurysm-related SAH (including traumatic); b) deceased patients before the intervention; c) patients who were transferred to other centers for intervention; and d) those who did not undergo any of these interventional approaches. The included participants were treated with each of the two approaches based on the consensus between the neurosurgical and interventional neuroradiology groups. All neurosurgical clippings were performed by one neurological surgeon (Rouzbeh Shams Amiri), and all endovascular coilings were placed by one interventional neuroradiologist (Rahim Kohansal).
Variables, data source, and measurement
All data were retrieved from patients’ medical records. The Hunt and Hess (H&H) and World Federation of Neurosurgical Societies (WFNS) classifications were used to assess the severity of the SAH based on the patient’s clinical condition. The patients were graded regarding radiological SAH findings based on the modified Fisher scale (mFS). Functional outcomes were evaluated according to the modified Rankin score (mRS). A good functional outcome was considered as an mRS≤2. We also extracted data regarding post-op complications, length of stay in hospital, length of stay in intensive care unit, and treatment cost.
Statistical methods
IBM SPSS software, version 21 (IBM Corporation, Armonk, NY, USA) was used for statistical analysis. Continuous variables were reported as Mean±SD, and categorical variables were reported as frequency (percentage). Continuous variables were compared using the independent t-test. Categorical variables were compared using the chi-square test or Fisher’s exact test. A P<0.05 was considered statistically significant.
3. Results
Baseline characteristics of the study participants
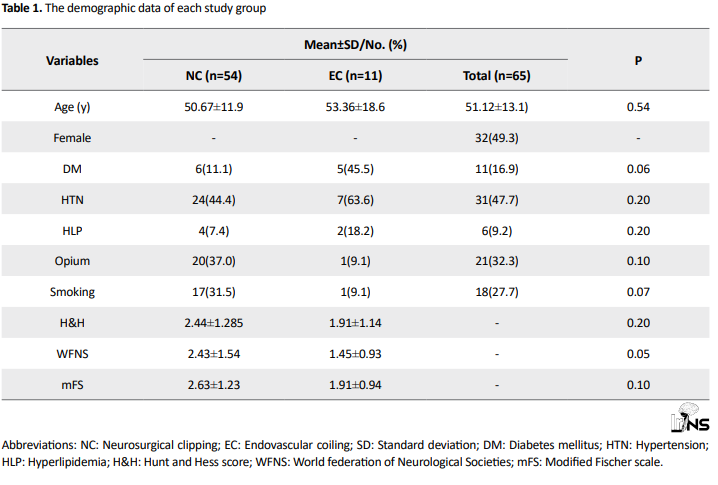
A total of 65 patients entered the study (mean age, 51.12±18.6 years old; 49.3% female), of whom 54 underwent neurological clipping and 11 were treated with endovascular coiling. Table 1 demonstrates the demographic data of each study group. There was no significant difference between the study groups regarding age, diabetes mellitus, hypertension, hyperlipidemia, opium consumption, and smoking. The mean H&H score was 2.44±1.28 in the neurosurgical group and 1.91±1.14 in the endovascular group. Likewise, the endovascular group had lower WFNS (mean, 2.43±1.54 vs 1.45±0.93) and mFS (mean, 2.63±1.23 vs 1.91±0.94) compared to the neurosurgical group. However, these differences were not significant (P=0.20, 0.05, and 0.10, respectively).
Outcomes and complications
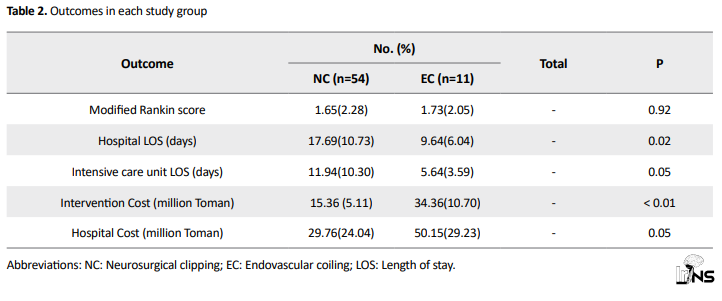
No significant relationship was detected between the mRS scores between the neurosurgical clipping group and the endovascular coiling group (1.65±2.28 vs 1.73±2.05; P=0.92). As shown in Table 2, the length of in-hospital stay was significantly lower in the endovascular group compared to the neurosurgical group (9.64±6.04 days vs 17.69±10.73 days; P=0.02). Likewise, the length of in-intensive care unit stay was lower in the coiling group compared to the clipping group (5.64±3.59 days vs 11.94±10.30 days); however, it was not significant (P=0.05). In contrast, intervention cost was significantly higher in the endovascular group compared to the neurosurgical group (34.36 million Toman ±10.70 vs 15.36 million Toman ±5.11; P<0.01). Hospital cost also was higher in the coiling group compared to the clipping group (50.15±29.23 million Toman vs 29.76±24.04 million Toman), still, it did not reach the level of significance (P=0.05).
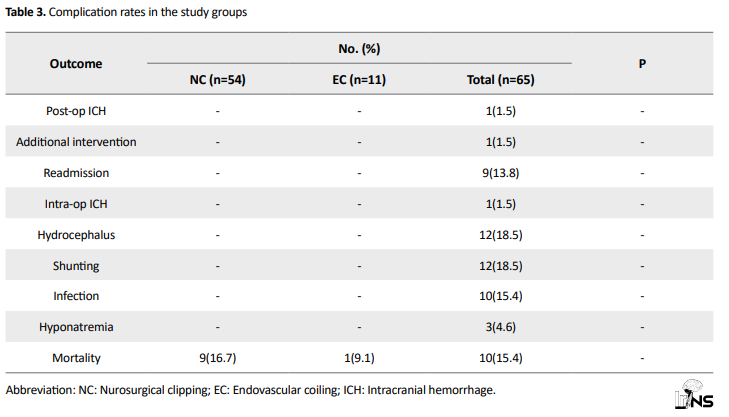
The mortality rate was not significantly different between the two study groups (Table 3). There was a total of 12 cases of hydrocephalus, all of which were shunted, and there was no difference between the two groups in this regard. Additionally, there was one case that experienced bleeding during coiling and subsequently underwent open surgery with a good outcome (mRS≤2).
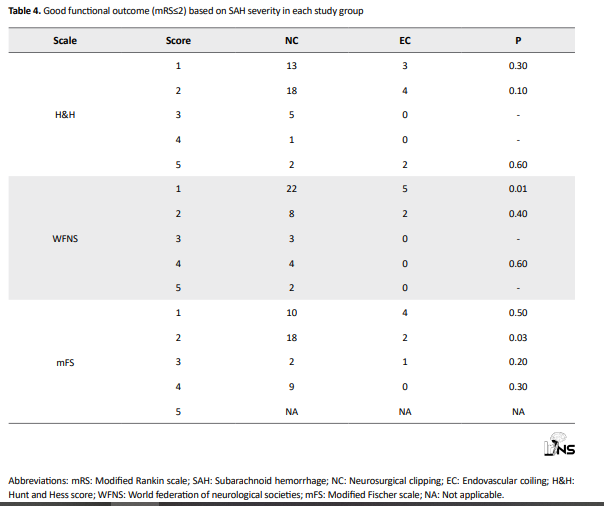
Subgroup analysis of good functional outcome (mRS≤2) based on the H&H score showed no significant differences (Table 4). We observed a significant difference between the two groups in WFNS score equal to one, in which 22 good functional outcomes were seen in the neurosurgical group compared to 5 in the endovascular group (P=0.01). Besides, there was a significant difference between the two groups in those with mFS scores equal to two; meanwhile, mRS≤2 was seen in 18 of 19 patients in the neurosurgical group compared to 2 of 5 patients in the endovascular group (P=0.03). Other scores did not reach the level of significance.
4. Discussion
The management of aneurysm-related SAH offers a significant challenge due to its life-threatening nature and potential for devastating consequences. In our retrospective cohort study, we compared the efficacy and outcomes of two conventionally employed treatment modalities for aneurysmal SAH, namely neurosurgical clipping and endovascular coiling. The findings validate existing literature in highlighting the severity and high mortality rates associated with aneurysmal SAH. This emphasizes the critical need for prompt intervention to alleviate the risk of rebleeding and improve patient outcomes. Both neurosurgical clipping and endovascular coiling serve as the main strategies in this regard, with distinct advantages and limitations [8].
Neurosurgical clipping was considered the gold standard intervention for a long time and involves the placement of a titanium clip via a craniotomy to isolate the aneurysm [9]. While it is considered an effective option in securing the aneurysm and reducing the risk of rebleeding, this approach is associated with expanded recovery times and heightened risks of complications. Conversely, endovascular coiling offers a less invasive alternative, wherein a platinum coil is delivered to the aneurysm via a microcatheter, building up intra-aneurysmal thrombosis and its closure. Our study suggests comparable efficacy between these two methods in preventing rebleeding and improving functional outcomes.
Notably, the present analysis revealed several key findings regarding the comparative outcomes of neurosurgical clipping versus endovascular coiling. While there were no significant differences in functional outcomes, as assessed by mRS, between the two groups, certain trends were observed. The patients undergoing endovascular coiling experienced shorter lengths of in-hospital and in-ICU stays, indicative of potentially faster recovery times and reduced healthcare and resource utilization .
However, it is essential to interpret these findings cautiously, considering the inherent biases associated with retrospective cohort studies and the limited sample size of our cohort.
Moreover, our study identified a significant disparity in intervention costs between neurosurgical clipping and endovascular coiling, with the latter demonstrating higher associated expenses. This economic consideration is paramount, particularly in resource-constrained healthcare settings, and warrants further exploration to inform cost-effective treatment strategies.
Subgroup analyses based on the H&H and WFNS classifications provided additional insights into the differential impacts of neurosurgical clipping and endovascular coiling on functional outcomes across varying disease severities. While no significant differences were observed in overall functional outcomes, subgroup analyses revealed nuanced distinctions, particularly in patients with WFNS scores of one and mFS scores of two. These findings underscore the importance of personalized treatment approaches tailored to individual patient characteristics and disease severity profiles.
As mentioned earlier, there is a discrepancy between the published studies regarding the most efficacious approach [10]. In a systematic review and meta-analysis conducted by Luo et al., five studies were assessed to overcome this issue. They found that endovascular coiling is superior to surgical clipping regarding functional outcome and cerebral ischemia. On the contrary, technical failure was more common in the endovascular group. They did not find any significant difference between the two groups regarding rebleeding and mortality [5]. In another systematic review and meta-analysis performed by Ahmed et al. 22 studies were included for meta-analysis. Despite the other review, they found that endovascular coiling is related to increased mortality rate, rebleeding, and retreatment. They showed that other complications are more prevalent in the clipping group; furthermore, more rehabilitation was needed in this group [4]. Jiang et al. [11] published an article in 2020 comprising 64 studies with different types. The study found that for subjects with ruptured aneurysms, clipping was correlated with a lower mortality and rebleeding rate in comparison with those who underwent coiling. However, between the clipping and coiling groups, the results were comparable regarding the rate of poor outcomes, ischemic infarct, or vasospasm.
For unruptured aneurysms, clipping was correlated with an increased risk of bad outcomes, but no significant difference was found in mortality compared to coiling. Clipping also decreased the rate of hydrocephalus and partial occlusion while increasing the complete occlusion rate for ruptured aneurysms. Considering only randomized controlled trials, clipping for ruptured aneurysms was associated with a higher rate of bad outcomes [11]. A recent study showed lower retreatments, incomplete occlusion, and short-term mortality rates in the neurosurgical group. Still, this approach was associated with higher ischemic infarction and longer length of stay [12].
Unlike many previously published articles in which different surgeons and neuro-interventionists performed the interventions, in our centers, only one physician performed the surgeries, and one did the interventions. This could minimize the risk of operator bias and result in more valid results. However, we should acknowledge the limitations of this study, including its retrospective nature, two-center design, indication for patient selection, and relatively small sample size .
Future prospective studies with larger sample sizes and longer follow-up durations are needed to validate our findings and provide more robust evidence to guide clinical decision-making.
5. Conclusion
This article contributes to the present research concerning the ideal management of aneurysmal SAH by comparing the outcomes and complications of the two major interventions. While both modalities demonstrate comparable efficacy in preventing rebleeding and improving functional outcomes, they present distinct advantages and considerations. A detailed understanding of patient-specific factors, disease severity, and economic implications is essential in selecting the most appropriate treatment strategy for individual patients. It seems that the best decision-making is either through teamwork between a neurovascular interventionist and a vascular-trained neurosurgeon, or by having the intervention performed by a hybrid vascular neurosurgeon. Future studies should be performed to improve treatment algorithms and patient outcomes in this complex clinical situation.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Golestan University of Medical Sciences, Gorgan, Iran (Code: IR.GOUMS.REC.1399.192). Informed consent was obtained from all participants/their families before their inclusion in the study.
Funding
This study was extracted from medical thesis of Ali Batiar, approved by Clinical Research Development Unit, Sayyad Shirazi Hospital, Golestan University of Medical Sciences, Gorgan, Iran.
Authors' contributions
Conceptualization and study design: Rouzbeh Shams Amiri and Seyed Aidin Sajedi; Data collection: Ali Batiar, Rouzbeh Shams Amiri and Rahim Kohansal; Data analysis and interpretation: Ali Batiar and Rouzbeh Shams Amiri; Drafting the article: Ali Batiar, Fateme Shahrokhi and Mohsen Nabiuni; Critically revising the article: Rouzbeh Shams Amiri, Mohammad Hossein Mirbolouk, Seyed Aidin Sajedi; Reviewing submitted version of manuscript: Rouzbeh Shams Amiri; Approving the final version of the manuscript: All authors.
Conflict of interest
The authors declared no conflict of interest.
References
Subarachnoid hemorrhage (SAH) due to aneurysmal rupture is a relatively common disease with a reported prevalence of 10 to 15 people per 100000 population in the USA [1]. Aneurysmal SAH is related to 30-day mortality rates of 80% to 100% compared to 33% to 50% in SAH overall [2]. This life-threatening condition is commonly diagnosed with a non-contrast brain computed tomography scan with or without diagnostic lumbar puncture [3]. Interventions are primarily trying to resuscitate the patient and reduce dependence in survivors. There are two common methods used for the treatment of SAH, trying to reduce rebleeding after SAH, including surgical clipping and endovascular coiling [4].
The gold standard intervention for SAH treatment is neurosurgical clipping [5]. This method is performed by clipping the aneurysm using a titanium clip and through access using a large craniotomy. Neurosurgical clipping results in an extended recovery time and is related to an increased risk of complications [5]. Minimally invasive methods, such as endovascular coiling, have been developed with advancements in interventional neuroradiology as an alternative treatment for aneurysmal SAH [6]. In this method, a platinum coil is attached to a microcatheter tip, which delivers it to the aneurysm lumen. Then, the coil is detached from the microcatheter, resulting in intra-aneurysmal thrombosis and its closure. Some studies suggest that the independence rate is higher in patients who were treated using endovascular coiling compared to neurosurgical clipping, with an increased risk of rebleeding in the coiling method [7]. However, there are contradictory results demonstrated by other studies regarding outcomes and complications [5].
There is a controversy between the studies regarding the efficacy and complications of each approach. Furthermore, these results could vary a lot in different settings and populations. To the best of our knowledge, no published investigation has been conducted comparing neurosurgical clipping and endovascular coiling in Iran. Therefore, this study compares these two conventional methods for aneurysmal SAH in our center with a focus on functional outcomes.
2. Materials and Methods
Study design and setting
This was a retrospective cohort study performed on consecutive patients with aneurysmal SAH who underwent either neurosurgical clipping or endovascular coiling at the Sayad-Shirazi or 5-Azar hospitals (both affiliated with Golestan University of Medical Sciences). The patients were referred for surgery from November 2016 to March 2021 and were followed up for two years. The medical records of each patient were extracted and were later used for comparison between the two approaches. This cohort was conducted adhering to the Declaration of Helsinki and its later amendments. We report the study based on strengthening the reporting of observational studies in epidemiology criteria for cohort studies.
Study participants
All patients afflicted with aneurysmal SAH who were referred to our two hospitals and were treated with either neurosurgical clipping or endovascular coiling were included in this cohort. The exclusion criteria were as follows: a) non-aneurysm-related SAH (including traumatic); b) deceased patients before the intervention; c) patients who were transferred to other centers for intervention; and d) those who did not undergo any of these interventional approaches. The included participants were treated with each of the two approaches based on the consensus between the neurosurgical and interventional neuroradiology groups. All neurosurgical clippings were performed by one neurological surgeon (Rouzbeh Shams Amiri), and all endovascular coilings were placed by one interventional neuroradiologist (Rahim Kohansal).
Variables, data source, and measurement
All data were retrieved from patients’ medical records. The Hunt and Hess (H&H) and World Federation of Neurosurgical Societies (WFNS) classifications were used to assess the severity of the SAH based on the patient’s clinical condition. The patients were graded regarding radiological SAH findings based on the modified Fisher scale (mFS). Functional outcomes were evaluated according to the modified Rankin score (mRS). A good functional outcome was considered as an mRS≤2. We also extracted data regarding post-op complications, length of stay in hospital, length of stay in intensive care unit, and treatment cost.
Statistical methods
IBM SPSS software, version 21 (IBM Corporation, Armonk, NY, USA) was used for statistical analysis. Continuous variables were reported as Mean±SD, and categorical variables were reported as frequency (percentage). Continuous variables were compared using the independent t-test. Categorical variables were compared using the chi-square test or Fisher’s exact test. A P<0.05 was considered statistically significant.
3. Results
Baseline characteristics of the study participants
A total of 65 patients entered the study (mean age, 51.12±18.6 years old; 49.3% female), of whom 54 underwent neurological clipping and 11 were treated with endovascular coiling. Table 1 demonstrates the demographic data of each study group. There was no significant difference between the study groups regarding age, diabetes mellitus, hypertension, hyperlipidemia, opium consumption, and smoking. The mean H&H score was 2.44±1.28 in the neurosurgical group and 1.91±1.14 in the endovascular group. Likewise, the endovascular group had lower WFNS (mean, 2.43±1.54 vs 1.45±0.93) and mFS (mean, 2.63±1.23 vs 1.91±0.94) compared to the neurosurgical group. However, these differences were not significant (P=0.20, 0.05, and 0.10, respectively).
Outcomes and complications
No significant relationship was detected between the mRS scores between the neurosurgical clipping group and the endovascular coiling group (1.65±2.28 vs 1.73±2.05; P=0.92). As shown in Table 2, the length of in-hospital stay was significantly lower in the endovascular group compared to the neurosurgical group (9.64±6.04 days vs 17.69±10.73 days; P=0.02). Likewise, the length of in-intensive care unit stay was lower in the coiling group compared to the clipping group (5.64±3.59 days vs 11.94±10.30 days); however, it was not significant (P=0.05). In contrast, intervention cost was significantly higher in the endovascular group compared to the neurosurgical group (34.36 million Toman ±10.70 vs 15.36 million Toman ±5.11; P<0.01). Hospital cost also was higher in the coiling group compared to the clipping group (50.15±29.23 million Toman vs 29.76±24.04 million Toman), still, it did not reach the level of significance (P=0.05).
The mortality rate was not significantly different between the two study groups (Table 3). There was a total of 12 cases of hydrocephalus, all of which were shunted, and there was no difference between the two groups in this regard. Additionally, there was one case that experienced bleeding during coiling and subsequently underwent open surgery with a good outcome (mRS≤2).
Subgroup analysis of good functional outcome (mRS≤2) based on the H&H score showed no significant differences (Table 4). We observed a significant difference between the two groups in WFNS score equal to one, in which 22 good functional outcomes were seen in the neurosurgical group compared to 5 in the endovascular group (P=0.01). Besides, there was a significant difference between the two groups in those with mFS scores equal to two; meanwhile, mRS≤2 was seen in 18 of 19 patients in the neurosurgical group compared to 2 of 5 patients in the endovascular group (P=0.03). Other scores did not reach the level of significance.
4. Discussion
The management of aneurysm-related SAH offers a significant challenge due to its life-threatening nature and potential for devastating consequences. In our retrospective cohort study, we compared the efficacy and outcomes of two conventionally employed treatment modalities for aneurysmal SAH, namely neurosurgical clipping and endovascular coiling. The findings validate existing literature in highlighting the severity and high mortality rates associated with aneurysmal SAH. This emphasizes the critical need for prompt intervention to alleviate the risk of rebleeding and improve patient outcomes. Both neurosurgical clipping and endovascular coiling serve as the main strategies in this regard, with distinct advantages and limitations [8].
Neurosurgical clipping was considered the gold standard intervention for a long time and involves the placement of a titanium clip via a craniotomy to isolate the aneurysm [9]. While it is considered an effective option in securing the aneurysm and reducing the risk of rebleeding, this approach is associated with expanded recovery times and heightened risks of complications. Conversely, endovascular coiling offers a less invasive alternative, wherein a platinum coil is delivered to the aneurysm via a microcatheter, building up intra-aneurysmal thrombosis and its closure. Our study suggests comparable efficacy between these two methods in preventing rebleeding and improving functional outcomes.
Notably, the present analysis revealed several key findings regarding the comparative outcomes of neurosurgical clipping versus endovascular coiling. While there were no significant differences in functional outcomes, as assessed by mRS, between the two groups, certain trends were observed. The patients undergoing endovascular coiling experienced shorter lengths of in-hospital and in-ICU stays, indicative of potentially faster recovery times and reduced healthcare and resource utilization .
However, it is essential to interpret these findings cautiously, considering the inherent biases associated with retrospective cohort studies and the limited sample size of our cohort.
Moreover, our study identified a significant disparity in intervention costs between neurosurgical clipping and endovascular coiling, with the latter demonstrating higher associated expenses. This economic consideration is paramount, particularly in resource-constrained healthcare settings, and warrants further exploration to inform cost-effective treatment strategies.
Subgroup analyses based on the H&H and WFNS classifications provided additional insights into the differential impacts of neurosurgical clipping and endovascular coiling on functional outcomes across varying disease severities. While no significant differences were observed in overall functional outcomes, subgroup analyses revealed nuanced distinctions, particularly in patients with WFNS scores of one and mFS scores of two. These findings underscore the importance of personalized treatment approaches tailored to individual patient characteristics and disease severity profiles.
As mentioned earlier, there is a discrepancy between the published studies regarding the most efficacious approach [10]. In a systematic review and meta-analysis conducted by Luo et al., five studies were assessed to overcome this issue. They found that endovascular coiling is superior to surgical clipping regarding functional outcome and cerebral ischemia. On the contrary, technical failure was more common in the endovascular group. They did not find any significant difference between the two groups regarding rebleeding and mortality [5]. In another systematic review and meta-analysis performed by Ahmed et al. 22 studies were included for meta-analysis. Despite the other review, they found that endovascular coiling is related to increased mortality rate, rebleeding, and retreatment. They showed that other complications are more prevalent in the clipping group; furthermore, more rehabilitation was needed in this group [4]. Jiang et al. [11] published an article in 2020 comprising 64 studies with different types. The study found that for subjects with ruptured aneurysms, clipping was correlated with a lower mortality and rebleeding rate in comparison with those who underwent coiling. However, between the clipping and coiling groups, the results were comparable regarding the rate of poor outcomes, ischemic infarct, or vasospasm.
For unruptured aneurysms, clipping was correlated with an increased risk of bad outcomes, but no significant difference was found in mortality compared to coiling. Clipping also decreased the rate of hydrocephalus and partial occlusion while increasing the complete occlusion rate for ruptured aneurysms. Considering only randomized controlled trials, clipping for ruptured aneurysms was associated with a higher rate of bad outcomes [11]. A recent study showed lower retreatments, incomplete occlusion, and short-term mortality rates in the neurosurgical group. Still, this approach was associated with higher ischemic infarction and longer length of stay [12].
Unlike many previously published articles in which different surgeons and neuro-interventionists performed the interventions, in our centers, only one physician performed the surgeries, and one did the interventions. This could minimize the risk of operator bias and result in more valid results. However, we should acknowledge the limitations of this study, including its retrospective nature, two-center design, indication for patient selection, and relatively small sample size .
Future prospective studies with larger sample sizes and longer follow-up durations are needed to validate our findings and provide more robust evidence to guide clinical decision-making.
5. Conclusion
This article contributes to the present research concerning the ideal management of aneurysmal SAH by comparing the outcomes and complications of the two major interventions. While both modalities demonstrate comparable efficacy in preventing rebleeding and improving functional outcomes, they present distinct advantages and considerations. A detailed understanding of patient-specific factors, disease severity, and economic implications is essential in selecting the most appropriate treatment strategy for individual patients. It seems that the best decision-making is either through teamwork between a neurovascular interventionist and a vascular-trained neurosurgeon, or by having the intervention performed by a hybrid vascular neurosurgeon. Future studies should be performed to improve treatment algorithms and patient outcomes in this complex clinical situation.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Golestan University of Medical Sciences, Gorgan, Iran (Code: IR.GOUMS.REC.1399.192). Informed consent was obtained from all participants/their families before their inclusion in the study.
Funding
This study was extracted from medical thesis of Ali Batiar, approved by Clinical Research Development Unit, Sayyad Shirazi Hospital, Golestan University of Medical Sciences, Gorgan, Iran.
Authors' contributions
Conceptualization and study design: Rouzbeh Shams Amiri and Seyed Aidin Sajedi; Data collection: Ali Batiar, Rouzbeh Shams Amiri and Rahim Kohansal; Data analysis and interpretation: Ali Batiar and Rouzbeh Shams Amiri; Drafting the article: Ali Batiar, Fateme Shahrokhi and Mohsen Nabiuni; Critically revising the article: Rouzbeh Shams Amiri, Mohammad Hossein Mirbolouk, Seyed Aidin Sajedi; Reviewing submitted version of manuscript: Rouzbeh Shams Amiri; Approving the final version of the manuscript: All authors.
Conflict of interest
The authors declared no conflict of interest.
References
- Shea AM, Reed SD, Curtis LH, Alexander MJ, Villani JJ, Schulman KA. Characteristics of nontraumatic subarachnoid hemorrhage in the United States in 2003. Neurosurgery. 2007; 61(6):1131-7. [DOI:10.1227/01.neu.0000306090.30517.ae] [PMID]
- de los Reyes K, Patel A, Bederson JB, Frontera JA. Management of subarachnoid hemorrhage with intracerebral hematoma: Clipping and clot evacuation versus coil embolization followed by clot evacuation. Journal of Neurointerventional Surgery. 2013; 5(2):99-103. [DOI:10.1136/neurintsurg-2011-010204] [PMID]
- van der Wee N, Rinkel GJ, Hasan D, van Gijn J. Detection of subarachnoid haemorrhage on early CT: Is lumbar puncture still needed after a negative scan? Journal of Neurology, Neurosurgery, and Psychiatry. 1995; 58(3):357-9. [DOI:10.1136/jnnp.58.3.357] [PMID]
- Ahmed SI, Javed G, Bareeqa SB, Samar SS, Shah A, Giani A, et al. Endovascular coiling versus neurosurgical clipping for aneurysmal subarachnoid hemorrhage: A systematic review and meta-analysis. Cureus. 2019; 11(3):e4320. [DOI:10.7759/cureus.4320] [PMID]
- Luo M, Yang S, Ding G, Xiao Q. Endovascular coiling versus surgical clipping for aneurysmal subarachnoid hemorrhage: A meta-analysis of randomized controlled trials. Journal of Research in Medical Sciences. 2019; 24:88. [DOI:10.4103/jrms.JRMS_414_18] [PMID]
- Koivisto T, Vanninen R, Hurskainen H, Saari T, Hernesniemi J, Vapalahti M. Outcomes of early endovascular versus surgical treatment of ruptured cerebral aneurysms. A prospective randomized study. Stroke. 2000; 31(10):2369-77. [DOI:10.1161/01.STR.31.10.2369] [PMID]
- Molyneux AJ, Kerr RS, Birks J, Ramzi N, Yarnold J, Sneade M, et al. Risk of recurrent subarachnoid haemorrhage, death, or dependence and standardised mortality ratios after clipping or coiling of an intracranial aneurysm in the International Subarachnoid Aneurysm Trial (ISAT): Long-term follow-up. The Lancet. Neurology. 2009; 8(5):427-33. [DOI:10.1016/S1474-4422(09)70080-8] [PMID]
- Lindgren A, Vergouwen MD, van der Schaaf I, Algra A, Wermer M, Clarke MJ, et al. Endovascular coiling versus neurosurgical clipping for people with aneurysmal subarachnoid haemorrhage.The Cochrane Database of Systematic Reviews. 2018; 8(8):CD003085. [DOI:10.1002/14651858.CD003085.pub3] [PMID]
- Molyneux AJ, Birks J, Clarke A, Sneade M, Kerr RS. The durability of endovascular coiling versus neurosurgical clipping of ruptured cerebral aneurysms: 18 year follow-up of the UK cohort of the International Subarachnoid Aneurysm Trial (ISAT). Lancet. 2015; 385(9969):691-7. [DOI:10.1016/S0140-6736(14)60975-2] [PMID]
- Calvanese F, Auricchio AM, Pohjola A, Hafez A, Nurminen V, Korja M, et al. Changes in treatment of intracranial aneurysms during the last decade in a large European neurovascular center. Acta Neurochirurgica. 2024; 166(1):173. [DOI:10.1007/s00701-024-06064-4] [PMID]
- Jiang Z, Chen Y, Zeng C, Feng J, Wan Y, Zhang X. Neurosurgical clipping versus endovascular coiling for patients with intracranial aneurysms: A systematic review and meta-analysis. World Neurosurgery. 2020; 138:e191-222. [DOI:10.1016/j.wneu.2020.02.091] [PMID]
- Peng L, Qin H, Liu J, Wu N, Wang X, Han L, et al. Neurosurgical clipping versus endovascular coiling for patients with ruptured anterior circulation aneurysms: A systematic review and meta-analysis. Neurosurgical Review. 2024; 47(1):68. [DOI:10.1007/s10143-024-02304-4] [PMID]
Type of Study: Research |
Subject:
Functional Neurosurgery
Send email to the article author
| Rights and Permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
